PART III- Choices for Communication Modalities
Karl R. White, PhD
National Center for Hearing Assessment and Management (NCHAM)
Utah State University
Special Note: This article is Part III of a 3-Part series modified for the OK Pediatrician E-Newsletter.
Part I – The Child’s Hearing Loss – can be located in the March – April 2019 publication:
http://www.okaap.org/wp-content/uploads/2019/03/OKAAP-MarchApril-2019-Newsletter-1.pdf
Part II – PART II– Hearing Status of the Parents – can be located in the May – June 2019 publication:
https://www.okaap.org/wp-content/uploads/2019/05/OKAAP-MayJune-2019-Newsletter.pdf
When determining effective service provision for children who are hard of hearing or deaf (HH/D), the primary care physician (PCP) must consider differences in variables such as the family’s ethnicity, education, religious and cultural beliefs, and family structure. These decisions are further complicated by the high degree of heterogeneity of children who are HH/D. The PCP must also consider the child’s hearing loss, hearing status of the parents, and parents’ choices for communication modalities of the child. Parts I and II focused on childhood hearing loss and the hearing status of parents. The PCP should also assist the family in considering communication options and helping them access the best possible support for however they choose to communicate with their child.
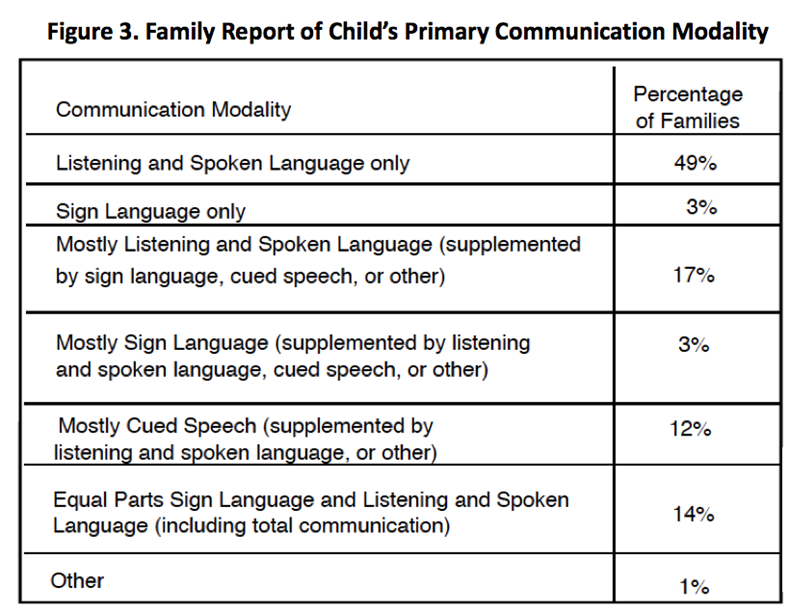
Communication Modalities Used by Families of Children Who Are HH/D: Families choose to communicate with their HH/D children in a variety of ways and the PCP should assist the family in considering these options. Based on currently available data, there is no “best way.” According to a recent national survey by NCHAM (EI SNAPSHOT, 2018b), a significant number of families explore multiple options during the child’s early years, and many change their approach or combine options from time to time. Figure 3 shows the percentage of families using various communication options in the EI SNAPSHOT sample. These findings are generally consistent with the Gallaudet’s 2011-2012 Annual Survey of Deaf and Hard of Hearing Children and Youth which reported that 51.8% of their respondents were taught using only spoken language, 15.5% using spoken language with Cues, 15.2% using sign language only, 13.2% with sign language and spoken language, and 4.2% with “other.”
The primary care physician is an essential part of team that enables children who are HH/D to reach their full potential. Achieving this goal requires that physicians recognize the heterogeneity of this population and the many options that families have for educating and communicating with their child who is HH/D.
REFERENCE:
National Center for Hearing Assessment and Management (NCHAM). (2018b). Early Intervention: Systematic Nationwide Analysis of Programs’ Strengths, Hurdles, Opportunities, and Trends (EI SNAPSHOT). Retrieved August 24, 2018 from http://www.infanthearing.org/ei-snapshot/docs/ei-snapshot-final-report.pdf